Auszug
Die Praxis Ortho4Sport in Köln, gegründet von Herrn Prof. Dr. med. Oliver Tobolski, setzt auf moderne, patientenorientierte Diagnostik. Bereits zur Eröffnung 2024 wurde sie mit dem SCS MedSeries® H22 ausgestattet – einer Technologie, mit der Herr Prof. Tobolski seit vielen Jahren arbeitet. Die hochauflösende 3D-Bildgebung liefert präzise Diagnosen bei minimaler Strahlendosis und steht binnen Sekunden zur Verfügung – ohne aufwendige Lagerung, mit hohem Komfort für den Patienten.
Auch das Praxisteam profitiert von der intuitiven Bedienung und schnellen Einarbeitung. Besonders schätzt Herr Prof. Tobolski die Möglichkeit, die plastischen 3D-Rekonstruktionen direkt im Gespräch mit dem Patienten einzusetzen – verständlich, anschaulich und auf Augenhöhe. Gerade bei komplexen Fällen liefert sie entscheidende Befunde – und ist für Ortho4Sport längst unverzichtbar: Medizinisch präzise, menschlich wertvoll und wirtschaftlich sinnvoll.
In einem Interview sprach er über die moderne Art zu diagnostizieren und welche Rolle die SCS MedSeries® in der konservativen Sportorthopädie spielt.

Maßgeschneiderte orthopädische Lösungen zur vollen Entfaltung des eigenen Potenzials – so lautet das Motto der fortschrittlichen Ortho4Sport, eine sportorthopädische Praxis in Köln. Gegründet wurde sie von Herrn Prof. Dr. med. Oliver Tobolski, der hier neueste medizinische Technologie mit erstklassiger Betreuung verbindet. Mit individuellen Therapieansätzen und einem engagierten, fachlich geschulten Team wird Menschen aller Altersgruppen dabei geholfen, in einen gesunden Alltag zurückzukehren. Um den hohen Ansprüchen des Arztes, des Teams und den Patienten gerecht zu werden, wurde die Ortho4Sport schon zur Praxiseröffnung mit der SCS MedSeries® H22 ausgestattet.
Als einer der DVT-Pioniere in der Humanmedizin arbeitete er bereits in einer anderen, renommierten Praxis mit dieser Technologie. Auch in der neuen Praxis, die er nun seit 2024 leitet, ist diese hochentwickelte Lösung im Einsatz. Gemeinsam mit dem Praxisteam sorgt Prof. Dr. med. Tobolski für eine individuelle und patientenorientierte Behandlung.
Innovative Diagnostik ist der gelebte Standard
Als einer der ersten Anwender der SCS Bildgebung kann Herr Prof. Tobolski auf viele Jahre Erfahrung zurückblicken. Die digitale Volumentomographie ist fest in seinem Praxisalltag verankert, weshalb es außer Frage stand, dieses Diagnostikverfahren auch in der Ortho4Sport einzusetzen und im vollen Umfang zu nutzen. Die Vorteile liegen für ihn ganz klar auf der Hand:
„Die SCS Bildgebung ist extrem patientenfreundlich, strahlenarm, höchst innovativ und sehr treffsicher in der Diagnostik.”
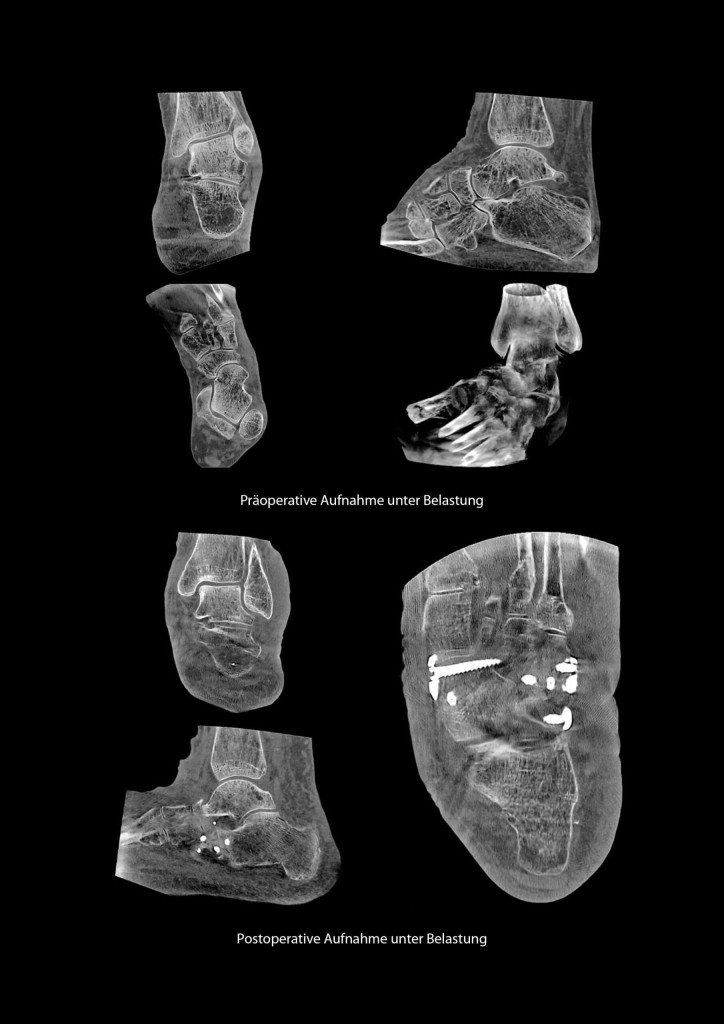
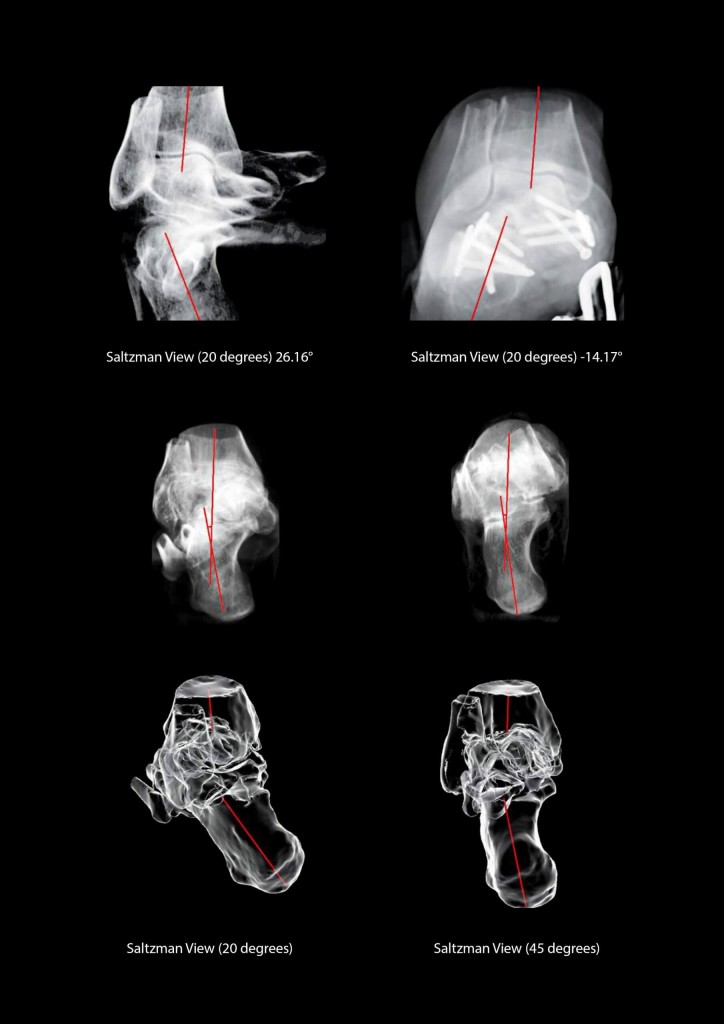
Mit dem eigenständigen Betrieb erzielt der Arzt schnell präzise Ergebnisse, auf deren Basis therapeutische Entscheidungen fundiert getroffen werden können. Dabei hilft die detaillierte, multiplanare Aufnahme in 0,2 mm Schichtdicke.
„Die Bildauflösung ist deutlich besser und genauer als eine Aufnahme mittels konventioneller Röntgenverfahren. Das hat direkten Einfluss auf die Aussagekraft der erstellen 3D-Schnittbilder und steigert meine Diagnosesicherheit enorm.”

Einfach im Alltag, sicher in der Handhabung
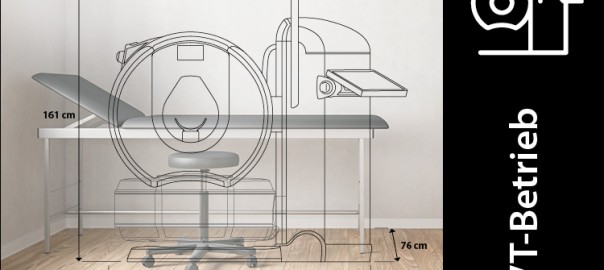
Er betont besonders, dass es sich um eine praxisorientierte Lösung handelt, die dem Team den Einstieg leicht macht, sich im Alltag schnell bewährt und zugleich durch ihre kompakte Bauweise überzeugt. Die gängigen Vorurteile, die dieser Technologie gelegentlich entgegengebracht werden – etwa ein hoher Schulungsaufwand oder ein zu großer Platzbedarf – hält Herr Prof. Tobolski für unbegründet.
Seine langjährige Erfahrung zeigt vielmehr das Gegenteil: Die Implementierung gelingt mühelos, die Handhabung ist für das gesamte Team verständlich und der Nutzen im Praxisalltag sofort spürbar.
„Die Implementierung in die eigene Praxis ist einfacher als bei einem MRT und die Bedienung des Systems wird problemlos durchgeführt. Daher kann ich Bedenken um eine zu teure Anschaffung mit zu großem Personalaufwand nicht bestätigen.“
Für den Facharzt ist klar: Die Investition amortisiert sich schnell – durch eine saubere, zielgerichtete Diagnostik, die das Vertrauen der Patienten stärkt und unnötige Umwege erspart. Eine solch qualitativ hochwertige Leistung wird von den Patienten sehr geschätzt und honoriert.
Diagnostik mit hoher Teamakzeptanz
Damit ein neues Diagnostikverfahren erfolgreich ist, braucht es die Akzeptanz des Teams. In der Ortho4Sport ist das SCS MedSeries® H22 fest etabliert und wird von den Mitarbeitern nicht nur als technische Erweiterung, sondern vor allem als spürbare Erleichterung im Alltag wahrgenommen. Besonders geschätzt werden die einfache Bedienung und die schnelle Verfügbarkeit der Aufnahmen. Das Feedback fällt daher durchweg positiv aus, berichtet Herr Prof. Tobolski.
„Die Arbeit mit der SCS Bildgebung fällt meinen Mitarbeitern sehr leicht, da das Verfahren schnell erlernbar und gut reproduzierbar ist. Die Bedienung ist innovativ und daher wenig fehleranfällig. Es gibt eine kurze Learning Curve und alle Mitarbeiter sind sehr schnell in der Lage, sehr gute Bildergebnisse zu erzielen, die in einer qualifizierte Befundung resultieren.“
Das Ergebnis überzeugt nicht nur das gesamte Praxisteam – sondern auch die Patienten. Die 3D-Schnittbilder liegen dem behandelnden Arzt innerhalb weniger Sekunden vor und können gemeinsam am Befundmonitor besprochen werden.
Kommunikation auf Augenhöhe
Die Möglichkeit, die Untersuchungsergebnisse direkt im Anschluss gemeinsam mit den Patienten zu besprechen und dabei die dreidimensionale Darstellung einzusetzen, verbessert das Arzt-Patienten-Verhältnis spürbar, erklärt Herr Prof. Tobolski.
Diesen Aspekt sieht er als entscheidend für die Patientenkommunikation an, denn die Transparenz sorgt für mehr Akzeptanz und stärkt die gemeinsame Therapieentscheidung. Gerade im Bereich der Sportorthopädie, in der Patienten häufig einen hohen Anspruch an Präzision und Selbstbestimmung mitbringen, ist das ein echter Mehrwert.
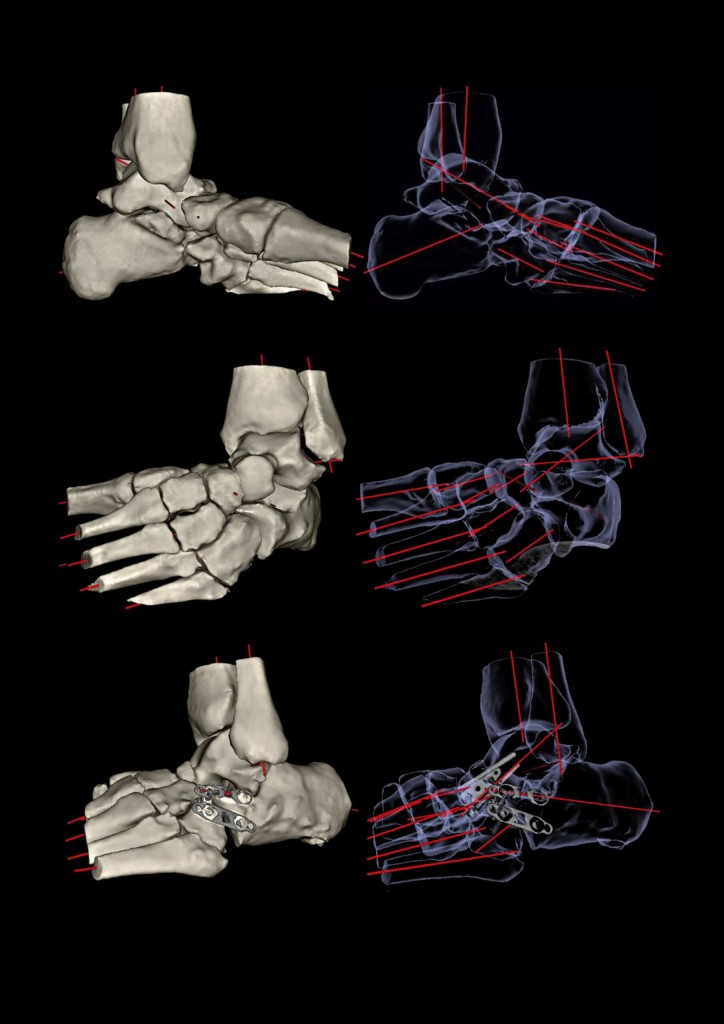
„Durch die 3D-Darstellung können wir dem Patienten Gelenke plastisch zeigen und Probleme detailliert visualisieren. Das ist für mich der wichtigste Punkt in der Nutzung dieses Verfahrens. Wenn der Patient seinen Befund versteht, erreichen wir eine sehr hohe Patientencompliance.”
Verborgenes sichtbar machen und die richtige Diagnose finden
Mit Blick auf vergangene Fälle, die Herrn Prof. Tobolski besonders im Gedächtnis geblieben sind, berichtet er über Patienten mit langanhaltenden und ausgeprägten Beschwerden – oft nach scheinbar harmlosen Unfällen. Sie haben bereits zahlreiche Schnittbildverfahren hinter sich, viele unterschiedliche Befunde, aber keine klare Diagnose.
Diese Fälle kommen immer häufiger auf Anfrage von Rechtsanwälten, da die Versicherungen solche Patienten nicht selten als „Simulanten“ einstufen – mit dramatischen Folgen für deren Versorgung und Lebensqualität. Hier eröffnet die hochauflösende 3D-Diagnostik neue Perspektiven, erzählt der Facharzt.
„Bei solchen Fällen hilft uns die moderne 3D-Schnittbildgebung ganz besonders. Strukturelle Veränderungen in den oberen Kopfgelenken des Dens axis und beginnende arthrotische Veränderungen können mit der SCS Bildgebung einwandfrei dargestellt werden, während sie in der herkömmlichen Diagnostik untergehen.“
Für viele dieser Patienten bedeuten die neuen Befunde nicht nur lang erhoffte Klarheit über die Ursachen ihrer Beschwerden, sondern eröffnen zugleich endlich den Zugang zur richtigen Therapie – oftmals nach einer langen Phase der Unsicherheit, zahlreicher Voruntersuchungen und fehlender Antworten.
„Die 3D-Diagnostik macht in solchen Fällen wirklich den großen Unterschied und ich freue mich, dass ich den Patienten helfen kann.”

Fazit: Ein Verfahren, das in der eigenen Praxis nicht fehlen darf
Für Herrn Prof. Oliver Tobolski hat sich die SCS Bildgebung vom diagnostischen Werkzeug zu einem festen Bestandteil seiner ärztlichen Identität entwickelt. Sie verbindet technische Präzision mit echter Patientenorientierung: Plastische 3D-Rekonstruktionen schaffen Transparenz, erleichtern die Kommunikation und fördern die Compliance. Gleichzeitig überzeugt die Lösung durch ihre Effizienz und Wirtschaftlichkeit.
Für das Team der Ortho4Sport steht fest: Die SCS Bildgebung ist integraler Bestandteil moderner Orthopädie und für jede Praxis ein unverzichtbarer Fortschritt. Auch nach vielen Jahren der Nutzung ist Herr Prof. Tobolski nach wie vor überzeugt, dass die SCS Bildgebung einen festen Platz in der modernen orthopädischen Diagnostik verdient.
Besonders im niedergelassenen Bereich – aber auch in Kliniken, in denen viele Kolleginnen und Kollegen das Potenzial des Verfahrens bislang nicht kennen.
„Mit der SCS Bildgebung kann ich komplexe Fälle, die zuvor im diagnostischen Graubereich blieben, mit hoher Sicherheit klären. Das hat auf die Therapie und die Lebensqualität meiner Patienten einen entscheidenden Einfluss. Ich lade jeden ein, sich diese Lösung einmal anzuschauen. Ich zeige es gerne vor Ort – denn die Kombination aus schneller Untersuchung, niedriger Strahlendosis und hoher Auflösung ist einfach zu gut, um sie ungenutzt zu lassen.“
Prof. Dr. Oliver Tobolski
Ortho4Sport
Industriestraße 161
50999 Köln
www.ortho4sport.de
Digitale Volumentomographie mit dem SCS MedSeries® H22
SCS steht für Sophisticated Computertomographic Solutions und beschreibt die Lösung für die anspruchsvolle 3D-Bildgebung mit höchster Strahlenhygiene, höchster Bildauflösung sowie höchster Zeitersparnis für Patient, Praxis und Arzt – als Win-Win-Win-Situation – gleichermaßen.
Der digitale Volumentomograph SCS MedSeries® H22 besitzt ein breites Indikationsspektrum und ist aus der Orthopädie und Unfallchirurgie nicht mehr wegzudenken. Mit dem platzsparenden Design findet das DVT in jeder Praxis einen Platz. Dank der hohen Strahlenhygiene und der Auflösung von bis zu 0,2 mm ist der digitale Volumentomograph auch in der Pädiatrie anwendbar. Die vom DVT ausgehende Strahlendosis kann unterhalb der täglichen terrestrischen Strahlendosis eingestellt werden und ist im Vergleich zur Computertomographie um bis zu 92 % geringer.
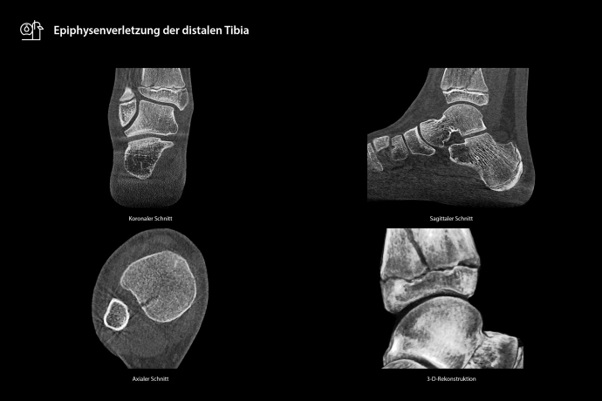
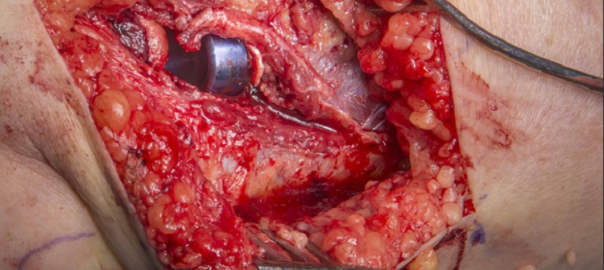
Die hochauflösenden Schnittbilder stehen, inklusive Rekonstruktionszeit, innerhalb von drei Minuten in multiplanarer Ansicht (axial, koronal, sagittal) sowie in 3D am Befundungsmonitor zur Beurteilung durch den behandelnden Arzt zur Verfügung. Im Resultat ist es mit dem DVT möglich, eine 3D-Schnittbilddiagnostik durchzuführen, die sehr strahlungsarm ist, eine exakte Beurteilung von Grenzflächen zwischen Metall- und Knochenstrukturen zulässt, und sehr einfach am Patienten anzuwenden ist.
Jetzt Beratungsangebot zum planungssicheren Einstieg in die SCS Bildgebung anfordern.